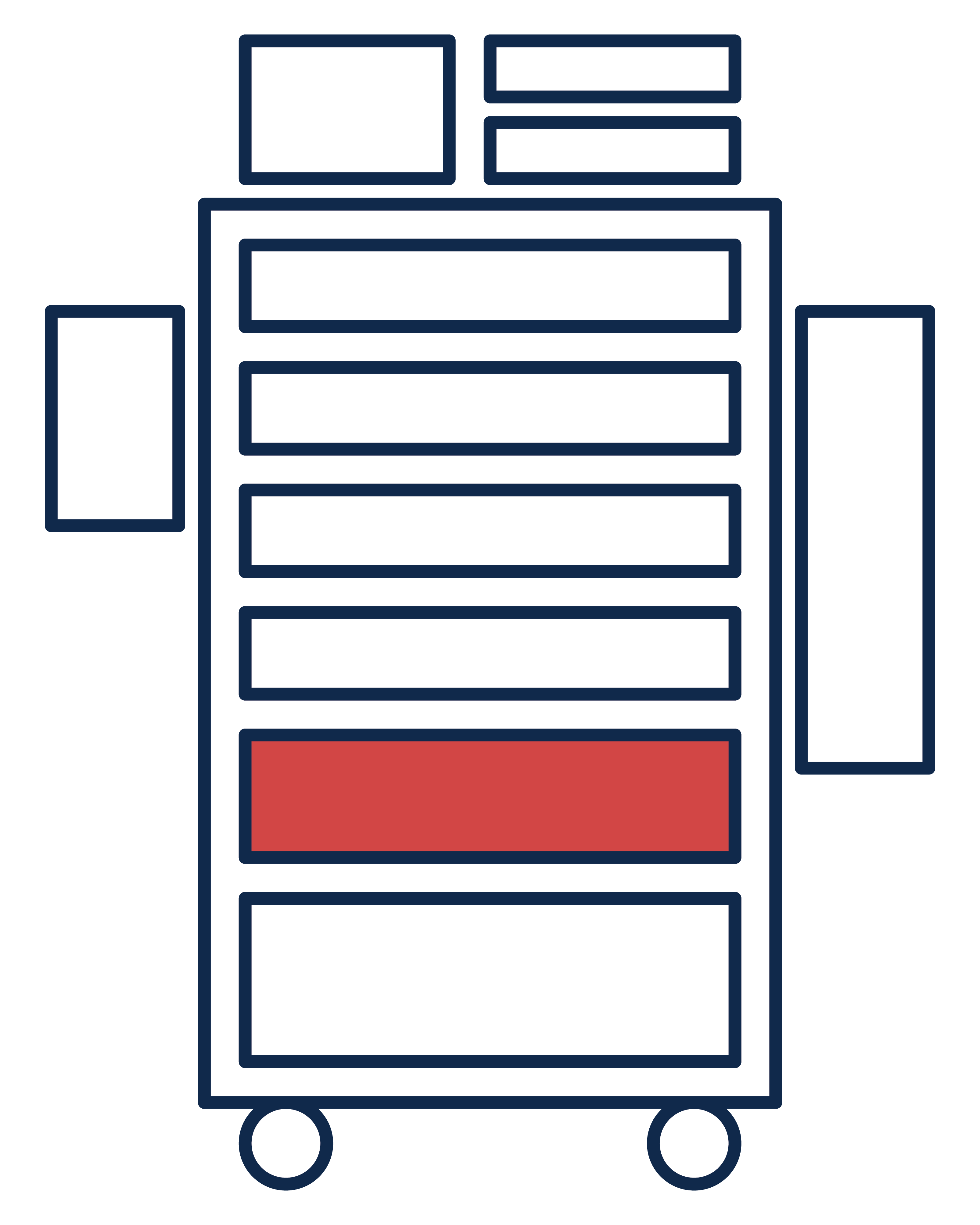
Drawer 1: Drugs
| Drug | Purpose | Mechanism of Action | Precautions | Use in Emergencies | |
|---|---|---|---|---|---|
| 1 | Naloxone (Narcan) 0.4 mg/ml | Reverses the effects of opioid overdose. | Pure opioid antagonist that competes and displaces opioids at opioid receptor sites. |
|
|
| 2 | Amiodarone (Cordarone) 150 mg vial | Treats acute life-threatening dysrhythmias, including ventricular tachycardia/fibrillation and supraventricular tachycardia. |
|
Avoid in patients with:
|
Administer undiluted over 10 minutes for the treatment of pulseless ventricular tachycardia/ventricular fibrillation unresponsive to CPR, defibrillation, and vasopressor therapy. |
| 3 | Adenosine 6 mg vial | Suppresses supraventricular tachycardia. | Slows conduction time through the AV node by interrupting the re-entry pathways and restoring normal sinus rhythm. |
Avoid in patients with:
|
|
| 4 | Norepinephrine 1 mg/mL in 4 mL vials | Increases blood pressure in patients with hypotension or shock who are not responsive to IV fluids. |
|
|
|
| 5 | Sodium chloride 0.9% 10-20 mL vial for drug dilution |
|
|
|
For fluid resuscitation, give 30 mL/kg IV within 1 hour. |
| 6 | Magnesium sulfate, 50% 2 mL vials (1 g/mL) |
|
|
|
IV infusion
|
| 7 | Epinephrine 0.1 mg/mL Abboject™ | Increases blood pressure or heart rate or treats type I allergic reactions, including anaphylaxis. |
|
No absolute contraindications to the use of epinephrine in a life-threatening situation. |
|
| 8 | Lidocaine 0.4% (4 mg/mL) in 250 mL bag | Treats life-threatening arrhythmias, particularly those that are ventricular in origin, such as those that occur during acute MI. |
|
Avoid in patients with:
|
Administer lidocaine injection IV at a rate of approximately 25 to 50 mg/min. |
| 9 | Dextrose 50% (dextrose 25% if treating pediatrics) | Corrects acute hypoglycemia. | Provides calories and fluid for patients unable to obtain an adequate oral intake. |
Avoid in patients with:
|
Administer as a slow IV push if patient has signs and symptoms consistent with profound hypoglycemia and/or measured blood glucose < 54 mg/dL. |
| 10 | Lidocaine, 2% (20 mg/mL) in 5 mL prefilled syringe | Treats life-threatening arrhythmias, particularly those that are ventricular in origin, such as those that occur during acute MI. |
|
Avoid in patients with:
|
Administer lidocaine injection IV at a rate of approximately 25 to 50 mg/min. |
| 11 | Atropine sulfate 1 mg Abboject™ | Increases the heart rate and is an antidote for cholinergic poisoning. |
|
|
Administer 1 mg as an IV push if patient has symptomatic bradycardia (< 50 beats per minute and hypotension, altered mental status, signs of shock or signs of acute heart failure) or signs and symptoms of cholinergic poisoning (titrated to an effective dose that stops secretions). |
| 12 | Dopamine (1.6 mg/mL in 250 mL or 500 mL bag) | Improves perfusion of vital organs and/or increases cardiac output. |
|
|
|
| 13 | Sodium bicarbonate 8.4% 1 mEq/mL in a 50 mL prefilled syringe |
|
|
|
For cardiac arrest with acidosis, administer a rapid IV dose of 200 to 300 mEq of bicarbonate, given as a 7.5% or 8.4% solution. |
| 14 | Epinephrine 1 mg/mL vial |
|
|
No absolute contraindications to the use of epinephrine in a life-threatening situation. | 1 mg in 250mL of NS or D5W administered at 0.1 to 0.5 mcg/kg/minute IV for severe symptomatic hypotension/shock unresponsive to volume resuscitation. |
| 15 | Calcium chloride 10% 100 mg/mL in a 10 mL prefilled syringe |
|
Moderates nerve and muscle performance via action potential excitation threshold regulation across calcium channels. |
|
|
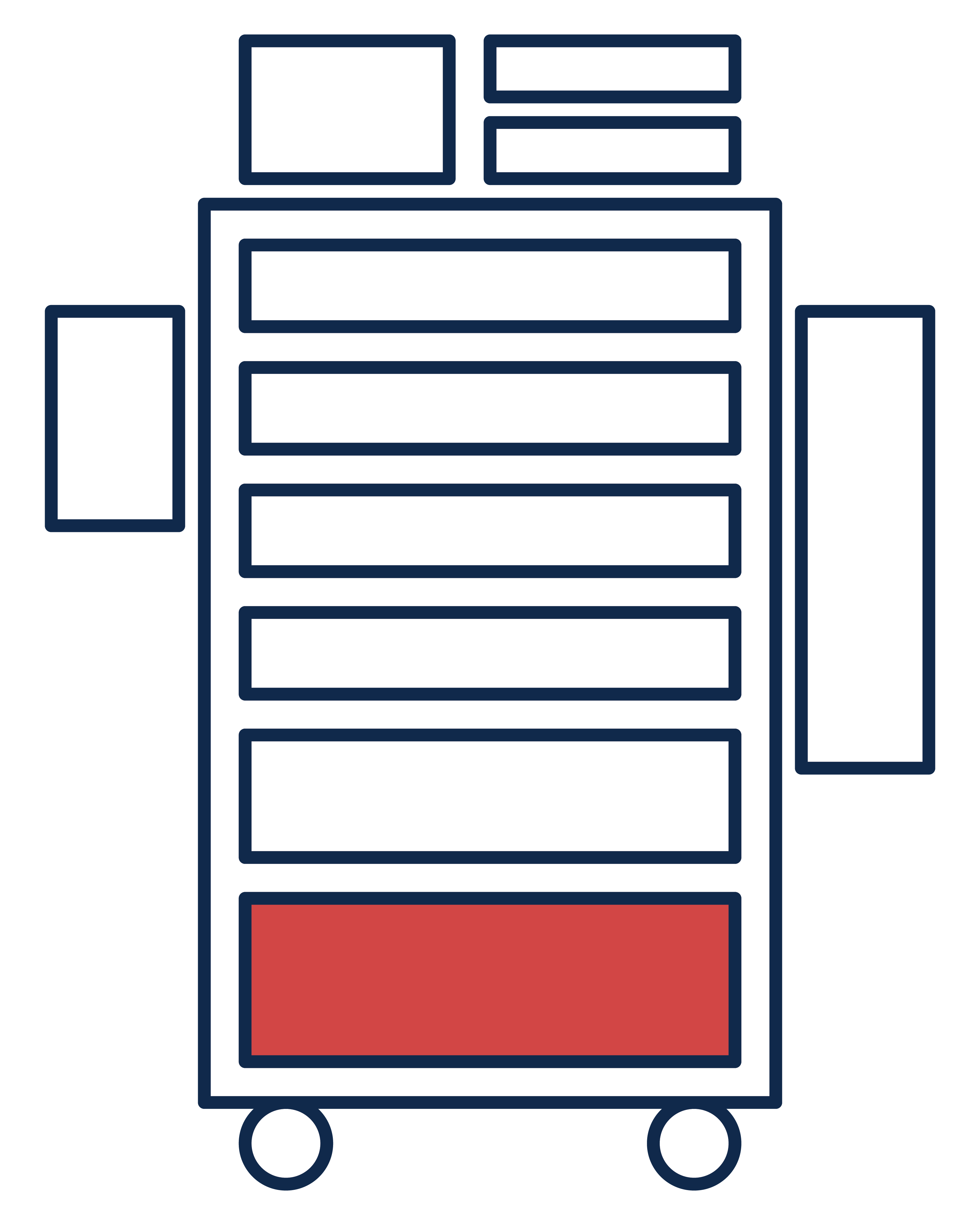
Drawer 2: Drugs
| Drug | Purpose | Mechanism of Action | Precautions | Use in Emergencies | |
|---|---|---|---|---|---|
| 1 | Aspirin 81 mg tablet |
|
|
Avoid in patients with known salicylate allergy, risk of bleeding, and in children with viral infections. | Chew and swallow two tablets. |
| 2 | Nitroglycerin spray or 0.4 mg sublingual tablets | Improves cardiac blood flow and reduces symptoms of angina. |
|
|
Administer sublingually if the patient has signs and symptoms consistent with angina or myocardial infarction. |
| 3 | Adult epinephrine auto injector (EpiPen) 0.3 mg | Increases blood pressure or heart rate or treats type I allergic reactions, including anaphylaxis. |
|
No absolute contraindications to the use of epinephrine in a life-threatening situation. | Administer 0.3 mg intramuscularly in patients having allergic reactions. Repeat every 5 to 15 minutes in the absence of clinical improvement. |
| 4 | Pediatric epinephrine auto injector (EpiPenJr) 0.15 mg | Increases blood pressure or heart rate or treats type I allergic reactions, including anaphylaxis. |
|
No absolute contraindications to the use of epinephrine in a life-threatening situation. | Administer 0.15 mg intramuscularly in pediatric patients (15-29 kg) having allergic reactions. Repeat every 5 to 15 minutes in the absence of clinical improvement. |
| 5 | Procainamide 1 g in 10 ml 100 mg/ml vial | Effective and recommended treatment alternative for hemodynamically stable monomorphic ventricular tachycardia in adults with preserved left ventricular function. |
|
Avoid in patients with known:
|
Administer 100 mg IV every 5 minutes until arrhythmia is controlled, hypotension occurs, or QRS complex widens by 50% of its original width. |
| 6 | Diltiazem 20 mg vial |
|
|
|
|
| 7 | Metoprolol 10 mg vial | Lowers blood pressure. |
|
Avoid in patients with known:
|
|
| 8 | Diphenhydramine (Benadryl) 50 mg vial | Blunts the effect of excess histamine. |
|
Avoid in patients with known hypersensitivity to diphenhydramine. |
|
| 9 | Methylprednisolone 125 mg vial | Reduces inflammation. |
|
Avoid in patients with known hypersensitivity to any component of the formulation (including those with milk allergies). |
|
Drawer 3: IV Supplies
Fluids and Tubing, Contents:
- Lactated Ringer's solution, 1000 mL
- 0.9% sodium chloride, 1000 mL
- 0.9% sodium chloride, 500 mL
- 5% dextrose, 100 mL
- 5% dextrose, 250 mL
- Blood tubing
- Primary IV tubing
Drawer 4: Pads & Leads
Pads & Leads, Box A Contents:
- Salem sump tubes
- NG tube holder
- Lubricant
- OG/NG syringe
- Scissors
- Kelly clamp
- Adhesive tape
- Waterproof tape
- Benzoin caps
Pads & Leads, Box B Contents:
- ECG patches
- Adult & ped defib pads
- Feedback pads
- Defib recording paper
- Pulse ox sensor
- Adult & child bp cuffs
Drawer 5: Procedures
Procedures, Box A Contents:
- Cricoid kit
- Cordis kit
- Chloraprep sponge
- Tegaderm
- Gauze sponge
- Sterile towels
- Sterile gloves
- Scalpel
Procedures, Box B Contents:
- A-line setup
- Femoral a-line kit
- 60 mL syringes
- Cardiac needle
- A-line cath
- Ear mask with shield
- Caps
Drawer 6: Suction & 02 Equipment
PPE & Suction, Side A Contents:
- Adult resuscitator kit
- Suction catheters
- IV pressure bags
- Oxygen adapter
- Non-rebreather mask
- Venti mask
- Bougie
- Oxygen connector
PPE & Suction, Side B Contents:
- Peds resuscitator kit
- Gowns
- Suction tubing
- 1200 cc canister with lid
- Nitrile gloves
- Suction regulator
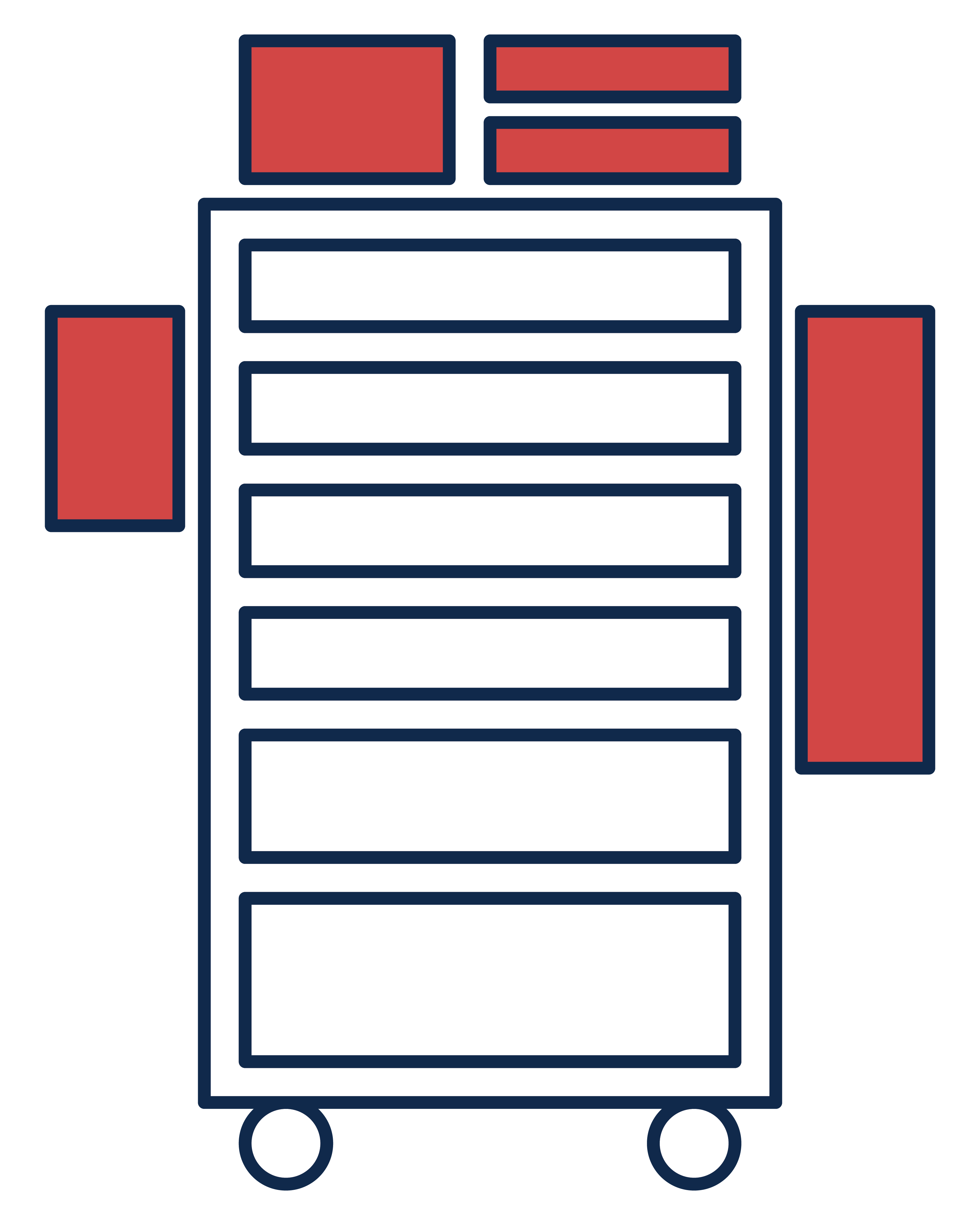
Cart Exterior
- Defibrillator
- 02 tank: gas oxygen size E with regulator
- Sharps container: sharps disposal 5.4 qt red
- Pediatric intubation kit
- Adult intubation kit